I have noticed that animal protection and animal rights are issues that unite people of many different backgrounds and political stripes (even more so than a love of nature or a desire to protect the environment). Most people recognize that we humans are animals too, and many people understand that all living beings have inherent value and should have the right to live and thrive.
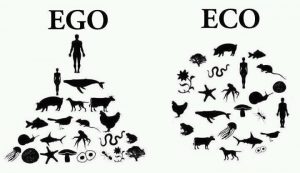
Personally, I believe that other species have as much of a right to exist, live, and thrive as humans do. I do not feel that my life has greater importance or value than the lives of other creatures. I also do not believe that other animals are here for us; they are here with us (and many species were here long before us), and they are not ours to use, abuse, commodify, cage, or exploit. Since they cannot speak for themselves or defend themselves against people (and our various types of weapons and threats), I do think it is our responsibility to try to protect them from other humans who do them harm.
Animals of all kinds—wild and domestic—face a wide variety of threats (to their survival, health, and well-being) from humans, including:
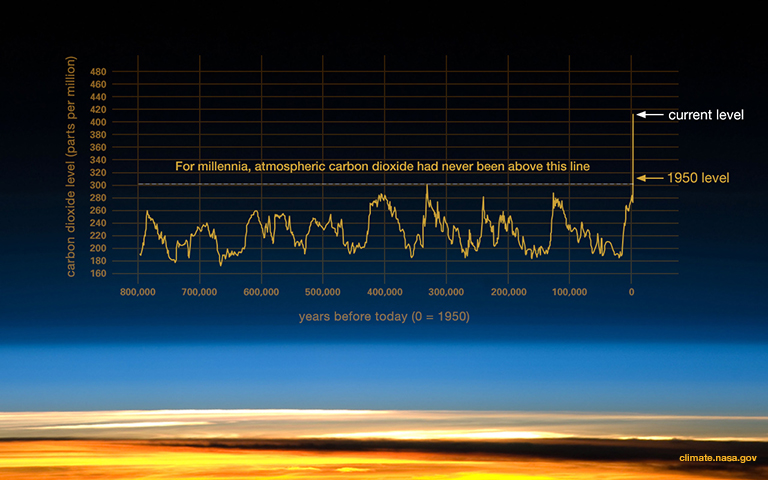
cruelty, abuse, domestic violence, neglect, exploitation and captivity (for human entertainment), factory farming, inhumane slaughter, over-hunting, poaching, trapping, trafficking, poisoning (e.g., rat poison and pesticides/herbicides; water, soil, and air pollution; plastic waste/pollution; intentional poisoning e.g. cyanide poisoning of elephants’ watering holes), widespread habitat destruction (e.g. from deforestation, development, agribusiness e.g. cattle grazing and crop plantations, mining, and road-building), medical research, animal testing (for products e.g. cosmetics), injury or death from vehicles or buildings (e.g., getting hit by cars or planes, birds flying into windows), and the overarching problem that affects all species including our own: climate change (extreme and volatile temperatures, drought; loss of food sources; extreme storms/hurricanes, flooding, fires, etc.)
Between 1970-2012 (in just over 40 years), humans have wiped out about 60% of the earth’s mammals, birds, fish, reptiles, and amphibians, according to WWF’s Living Planet report of 2018. (As the human population has increased, wildlife populations have decreased, by similar degrees. Over that same time period (1970-2012), the world population of humans almost doubled, growing by approx. 3.5 billion people to more than 7 billion people. In 2020, we’re now approaching 8 billion.) The WWF study also found that freshwater wildlife populations have decreased by 83%, and extreme deforestation in South and Central America has led to a wildlife decline of 89% in that region. During the past 12,000 years of human civilization, humans have killed almost half of the trees on earth; around 15 billion trees are cut down each year (source). When we destroy animals’ habitat, we are destroying living beings and biodiversity. This not only creates a bleaker world in which to live; we are also destroying our own cousins and our shared life support systems.
“The greatness of a nation and its moral progress can be judged by the way its animals are treated. …I hold that the more helpless a creature, the more entitled it is to protection by man from the cruelty of man.”
– Mahatma Gandhi
Below is a listing of some of the many organizations that advocate for animals. They include animal rights, welfare/protection, conservation, rescue and rehabilitation, and refuge/sanctuary groups. Some are focused primarily on wildlife (including threatened or endangered species, or biodiversity), while others are focused on domesticated / companion animals (e.g. pets) or farmed animals. And a few do work that addresses all of the above. I have mostly included groups with a national (U.S.) or international scope, but there are many local and regional community-based groups for animals (in particular rescue groups that serve a local area), as well. I encourage you to do an online search to identify and support the ones in your region. Also follow our Twitter list of animal protection groups.
Organizations are listed below under the categories: General/Broad-based; Biodiversity; Farm Animals (and Humane Eating); Wild Animal Sanctuaries; Anti-Poaching and -Trafficking; Species-Specific (elephants, wolves, marine animals, primates, donkeys); Disaster Response/Rescue; Anti- Animal-Testing/Research/Experiments; Petitions; Books, Films, Audio, Videos; and Other Resources. And at the end, you will see More Quotations and Related Posts.
Note: This listing is not comprehensive. Also, I cannot vouch for the effectiveness or integrity of every group listed here (i.e., being listed does not necessarily constitute an endorsement). I will periodically add more links to the listing as I learn about other interesting groups. Please feel free to recommend additional groups in the Comments section.
General / broad-based animal rights and welfare groups
Biodiversity groups
These groups focus on broad issues that affect wild animal populations, such as habitat conservation, wildlife and endangered species protection, biodiversity, rewilding, and climate.
Also see the Anti-poaching category below.
And see the land/habitat conservation groups listed in our post Sustainable Land Use and Land Stewardship.
Organizations that work to protect and preserve wilderness (including intact forests and other wild lands) are thereby also preserving habitat for wildlife.
Farm animal groups and rescues/sanctuaries
There are many animal rescues and sanctuaries all over the country and the world. The following list is just a small selection of them that provide safe places for farm(ed) animals. Do a search to find the ones in your area, and see if you can go on a tour, or donate / sponsor (“adopt”) an animal:
- Gentle Barn, MO, TN, and CA
- Farm Sanctuary, NY and CA
- Hope Animal Sanctuary, MS
- Barn Sanctuary, MI
- Wild Earth Farm and Sanctuary, KY
- Lighthouse Farm Sanctuary, OR
- Wildwood Farm Sanctuary & Preserve, OR
- Animal Place, CA
- Rancho Compasión, a farmed animal sanctuary, CA
- Goatlandia Farm Animal Sanctuary, CA
Humane eating/meat standards:
Some would (maybe rightly) argue that there is no such thing as “humanely” raising or slaughtering (or hunting) animals for meat. I have included vegetarian/vegan resources here, as well as information about the various “humane” standards and certifications for meat producers. While I believe the choice to be vegan or vegetarian is admirable and ideal, the reality is that most humans have been and continue to be carnivores (omnivores), and I don’t think that people can be shamed out of meat-eating. Non-dogmatically-presented information and education can help, and more people are moving towards a low-meat, more humanely-raised-meat, or no-meat (or dairy) diet, but those are choices that each person comes to based on their own personal convictions and experiences.
Wild/large animal sanctuaries
There are many others. To find others, check out this listing of accredited sanctuaries.
Also see the sanctuaries for specific species, e.g., elephants, wolves, donkeys, etc., listed under “Species-specific groups,” below.
Anti-poaching, -trafficking, -wildlife-crime groups
Species-specific groups
The following is a small selection of the many groups that focus on particular species:
Elephants:
(Also see the Anti-Poaching groups listed above, which help protect elephants as well as other animals. And see the films Love and Bananas, and Last Days of Ivory.)
Wolves:
Marine animals:
Find other marine animal rescue groups here (a listing). And see the films The Cove and Blackfish.
Primates:
Donkeys:
Big cats:
Disaster response/rescue groups
Do an online search to find out if there’s some type of Animal Disaster Response group, such as an Animal Response Team (e.g., “State Animal Response Team” (SART) or “Community/County Animal Response Team” (CART)) established in your state, county, or city/town. If there isn’t one, consider organizing people to start one in your area, to help rescue pets, horses, livestock, and other animals during disasters.
Anti- animal testing/research/experiments groups
Petitions
Many of the organizations listed in the first section and in other sections of this post create their own petitions or letters that you can sign on to. Sign up for some organizations’ mailing lists, and check their websites’ Action-related sections.
Also see these websites:
And you can also check these other petition sites, which sometimes have animal-related petitions.
Books, Films, Audio, Videos, Podcast
Books:
- Our Wild Calling: How connecting with animals can transform our lives—and save theirs, by Richard Louv
- Beyond Words: What Animals Think and Feel, by Carl Safina
- An Immense World: How Animal Senses Reveal the Hidden Realms Around Us, by Ed Yong
- The Sixth Extinction: An Unnatural History, by Elizabeth Kolbert
- The Great Animal Orchestra, by Bernie Krause
- Sy Montgomery’s books, including Tamed and Untamed; The Soul of an Octopus; How to Be a Good Creature; etc.
- Jane Goodall’s books
- Animal Wise: How We Know Animals Think and Feel, by Virginia Morrel
- In Defense of Animals: The Second Wave, edited by Peter Singer
- Peter Singer’s books: The Ethics of What We Eat, and Animal Liberation
- Righteous Porkchop: Finding a Life and Good Food Beyond Factory Farms, by Nicolette Hahn Niman
- Feral: Rewilding the Land, the Sea, and Human Life, by George Monbiot
- Half-Earth: Our Planet’s Fight for Life, by Edward O. Wilson
- Other books on animal rights
Films:
Audio (natural/animal sounds):
Videos / social media:
Other Resources
Find wildlife rescue/rehabilitation centers in your state or county (and here’s another directory) — places that help treat orphaned, sick, or injured wildlife
Wildlifeel at Home: A conservation-based home design/build studio
Find domestic animal rescues/shelters for pet adoption near you
Dog Food Advisor (including pet food Recall alerts)
Dog Food Analysis
House Rabbit Society
Also see/follow our Twitter list of animal protection groups.
More Quotations
“We can judge the heart of a man by his treatment of animals.”
— Immanuel Kant
“What is man without the beasts? If all the beasts were gone, men would die from the great loneliness of spirit. For whatever happens to the beasts, soon happens to man. All things are connected.”
– widely attributed to Chief Seattle (but it actually seems to have been written or adapted by the screenwriter for the 1972 film Home)
“Our task must be to widen our circle of compassion to embrace all living creatures and the whole of nature in its beauty.”
— Albert Einstein
“We are forever responsible for that which we have tamed.”
– Antoine de Saint-Exupery
Related posts:
- Flea and Tick Treatments that Won’t Poison Your Pet
- Extreme Heat Health, Safety, and Survival: Tips for Helping People, Other Animals, and Plants
- Sustainable Land Use and Land Stewardship
- Re-Tree the World
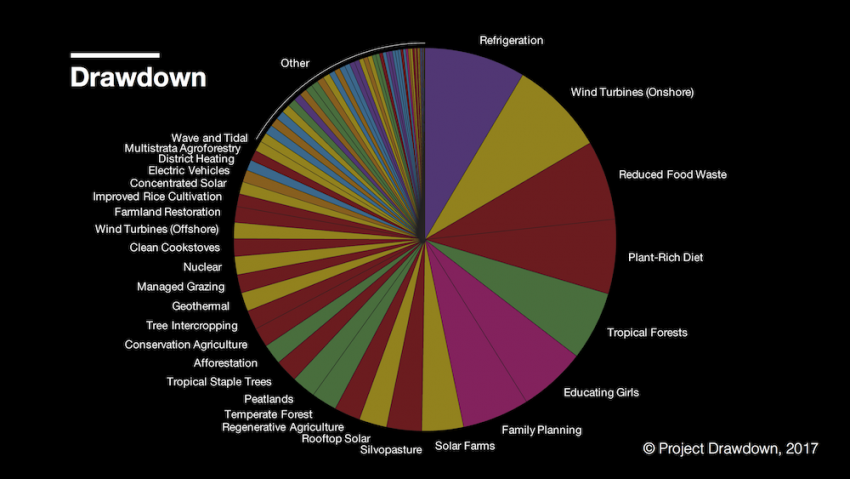
- The Most Effective Climate Strategies
- Climate Solutions, Tips, and Resources
- Sustainable Agriculture, Farming, Food-Related Resources
- Law Groups and Legal Frameworks for the Common Good
- A Few Good, Green Groups: Sustainability Organizations
- Natural Mosquito Control
- Get Ready, Be Ready: Tips for Emergency Preparedness and Disaster Response
- Our Tinderbox World: Wildfire Prevention and Risk Reduction
- State by State Voting Information
July 8, 2020
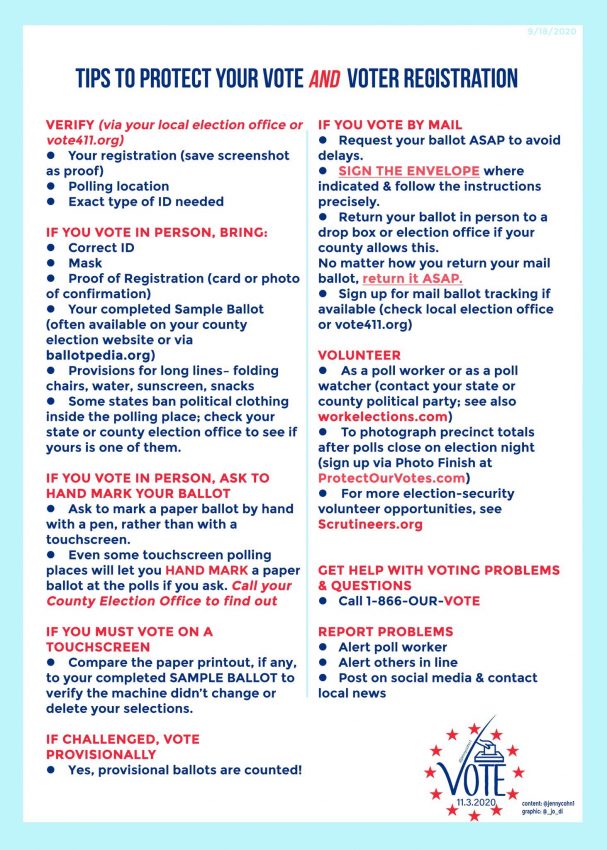
 So much is at stake in the next election (climate, democracy, Rule of Law, voting rights, women’s personhood, health and reproductive rights, etc.). Please double-check to make sure you’re registered to vote (and your registration information is accurate and up to date), then vote (early—in person or by mail, if those are options where you are), and encourage and help others you know to vote—and to make sure they have the required type of ID—especially young or first-time voters or people who have moved. (If you vote by mail, read all instructions very carefully, sign where indicated, and make sure your signature is representative of your official signature so it should closely match the signature they have on file and is not likely to be rejected. Drop it off at an official drop-off location, or mail it in well before the deadline so it will arrive in time. Make sure you use adequate postage, if postage is required. Then check with your county or state elections office for verification that it was received and counted.)
So much is at stake in the next election (climate, democracy, Rule of Law, voting rights, women’s personhood, health and reproductive rights, etc.). Please double-check to make sure you’re registered to vote (and your registration information is accurate and up to date), then vote (early—in person or by mail, if those are options where you are), and encourage and help others you know to vote—and to make sure they have the required type of ID—especially young or first-time voters or people who have moved. (If you vote by mail, read all instructions very carefully, sign where indicated, and make sure your signature is representative of your official signature so it should closely match the signature they have on file and is not likely to be rejected. Drop it off at an official drop-off location, or mail it in well before the deadline so it will arrive in time. Make sure you use adequate postage, if postage is required. Then check with your county or state elections office for verification that it was received and counted.)
 Studies have shown that exposure to various environmental toxins—which people can be exposed to via the air, water, soil, or the use of certain products—seem very likely to contribute to the development of a number of neurological and neurodegenerative disorders and diseases (including Alzheimer’s, other types of dementia, Parkinson’s disease, ALS, MS) and can also harm neurological development (e.g., intelligence) in children and babies’ developing brains.
Studies have shown that exposure to various environmental toxins—which people can be exposed to via the air, water, soil, or the use of certain products—seem very likely to contribute to the development of a number of neurological and neurodegenerative disorders and diseases (including Alzheimer’s, other types of dementia, Parkinson’s disease, ALS, MS) and can also harm neurological development (e.g., intelligence) in children and babies’ developing brains. This is a listing of some legal organizations that I recommend following, learning more about, and potentially supporting. They all use the law to try to serve and support the common good in various ways: to protect humans and human rights, civil rights, and civil liberties; to protect animals and the rights of non-human species; and/or to protect nature, our shared environment, and the livability of our planet.
This is a listing of some legal organizations that I recommend following, learning more about, and potentially supporting. They all use the law to try to serve and support the common good in various ways: to protect humans and human rights, civil rights, and civil liberties; to protect animals and the rights of non-human species; and/or to protect nature, our shared environment, and the livability of our planet.
 Over the past 10-15 years, it’s felt like new, large-scale crises emerge almost every day. It’s hard to focus on or prioritize any one issue, as so many issues are of dire importance.
Over the past 10-15 years, it’s felt like new, large-scale crises emerge almost every day. It’s hard to focus on or prioritize any one issue, as so many issues are of dire importance. We all have so many personal responsibilities and daily struggles and stressors of our own that it can be very hard to take in what’s going on in other people’s lives and in other parts of the world. Many people turn away because they are already overwhelmed and are in survival mode, and simply can’t cope with or absorb any more sad or scary news or more problems that seem intractable; we all go through certain periods of our lives, or parts of our days, when our own problems (or our families’) are all (or more than) we can handle. Taking on the weight of the world can be crushing. Almost none of us are unscathed or truly OK these days, as most of us are facing numerous challenges at societal and individual levels. It’s important to “put your own oxygen mask on first, before helping others with theirs” because you can’t help others unless you are alive, relatively sane and healthy, and able to function. But whenever we do have the capacity, we should strive to be compassionate, stay aware of what is going on outside of our immediate lives and circumstances, and try to make a difference whenever and wherever we can, however small our efforts may seem, on whatever specific issue(s) we feel we can make an impact on. Helping others (and humanity at large) also gives our own lives a greater sense of meaning and purpose.
We all have so many personal responsibilities and daily struggles and stressors of our own that it can be very hard to take in what’s going on in other people’s lives and in other parts of the world. Many people turn away because they are already overwhelmed and are in survival mode, and simply can’t cope with or absorb any more sad or scary news or more problems that seem intractable; we all go through certain periods of our lives, or parts of our days, when our own problems (or our families’) are all (or more than) we can handle. Taking on the weight of the world can be crushing. Almost none of us are unscathed or truly OK these days, as most of us are facing numerous challenges at societal and individual levels. It’s important to “put your own oxygen mask on first, before helping others with theirs” because you can’t help others unless you are alive, relatively sane and healthy, and able to function. But whenever we do have the capacity, we should strive to be compassionate, stay aware of what is going on outside of our immediate lives and circumstances, and try to make a difference whenever and wherever we can, however small our efforts may seem, on whatever specific issue(s) we feel we can make an impact on. Helping others (and humanity at large) also gives our own lives a greater sense of meaning and purpose.